Increase in Invasive Serogroup Y Meningococcal Disease in the United States

Distributed via the CDC Health Alert Network
March 28, 2024, 1:30 PM ET
CDCHAN-00505
Summary
The Centers for Disease Control and Prevention (CDC) is issuing this Health Alert Network (HAN) Health Advisory to alert healthcare providers to an increase in invasive meningococcal disease, mainly attributable to Neisseria meningitidis serogroup Y (Figure). In 2023, 422 cases were reported in the United States, the highest annual number of cases reported since 2014. As of March 25, 2024, 143 cases have been reported to CDC for the current calendar year, an increase of 62 cases over the 81 reported as of this date in 2023. A specific meningococcal strain, sequence type (ST) 1466, is responsible for most (101 of 148, 68%) serogroup Y cases with available sequence type data that were reported across the United States in 2023. Cases caused by this strain are disproportionately occurring in people ages 30–60 years (65%), Black or African American people (63%), and people with HIV (15%). In addition, most cases of invasive meningococcal disease caused by ST-1466 in 2023 had a clinical presentation other than meningitis: 64% presented with bacteremia, and at least 4% presented with septic arthritis. Of 94 patients with known outcomes, 17 (18%) died; this case-fatality rate is higher than the historical case-fatality rate of 11% reported for serogroup Y cases in 2017–2021. Healthcare providers should 1) have a heightened suspicion for meningococcal disease, particularly among populations disproportionately affected by the current increase, 2) be aware that patients may present without symptoms typical of meningitis, and 3) ensure that all people recommended for meningococcal vaccination, including people with HIV, are up to date for meningococcal vaccines.
Background
Meningococcal disease, caused by the bacterium Neisseria meningitidis, is a rare but severe illness with a case-fatality rate of 10–15% even with appropriate antibiotic treatment. Meningococcal disease most often presents as meningitis, with symptoms that may include fever, headache, stiff neck, nausea, vomiting, photophobia, or altered mental status; or as meningococcal bloodstream infection, with symptoms that may include fever and chills, fatigue, vomiting, cold hands and feet, severe aches and pains, rapid breathing, diarrhea, or, in later stages, a dark purple rash. While initial symptoms of meningococcal disease can at first be non-specific, they worsen rapidly, and the disease can become life-threatening within hours. Immediate antibiotic treatment for meningococcal disease is critical. Survivors may experience long-term effects such as deafness or amputations of the extremities.
Of the six N. meningitidis serogroups — A, B, C, W, X, and Y — responsible for most meningococcal disease worldwide, the four serogroups B, C, W, and Y circulate in the United States. Vaccines against serogroups A, C, W, Y (MenACWY) and serogroup B (MenB) are available in the United States. MenACWY vaccines are routinely recommended for adolescents and for people with other risk factors or underlying medical conditions, including HIV.
Across the United States, 101 ST-1466 cases were reported in 2023. This number is expected to increase with additional laboratory testing data. Cases of invasive meningococcal disease caused by this strain occurred in both males (65%) and females (35%) and disproportionately occurred in people ages 30–60 years (65%), Black or African American people (63%), and people with HIV (15%). In addition, most cases of invasive meningococcal disease caused by ST-1466 had a clinical presentation other than meningitis: 64% presented with bacteremia, and at least 4% presented with septic arthritis. Of 94 patients with known outcomes, 17 (18%) died; this case-fatality rate is higher than the historical case-fatality rate of 11% reported for serogroup Y cases in 2017–2021.
The serogroup Y ST-1466 strain has contributed to previously reported increases in meningococcal disease in people with HIV. Based on updated surveillance data, 24 ST-1466 cases have now been reported in people with HIV in 2022–2023; only four were previously vaccinated with MenACWY and none were up to date on recommended doses. To date, no other ST-1466 cases have been identified in people who previously received MenACWY vaccine.
Serogroup Y ST-1466 isolates tested to date have been susceptible to all first-line antibiotics recommended for treatment and prophylaxis. This strain is distinct from ciprofloxacin-resistant serogroup Y strains that are also circulating in the United States and that are disproportionately affecting Hispanic individuals.
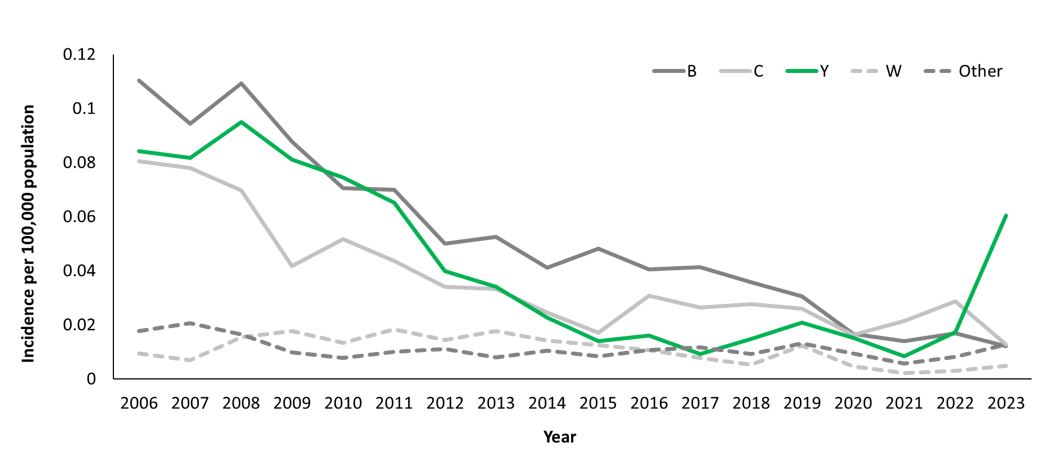
Figure: Trends in meningococcal disease incidence per 100,000 population, by serogroup—United States, 2006–2023. Incidence of Neisseria meningitidis serogroup Y is shown in green. Source: National Notifiable Diseases Surveillance System, with additional serogroup data from Active Bacterial Core surveillance (ABCs) and state health departments. 2022 and 2023 data are preliminary.
Recommendations for Public Health Departments
- Ensure healthcare providers are aware of the increasing burden of invasive meningococcal disease, particularly among people ages 30–60 years and Black or African American people.
- Continue submitting all meningococcal isolates to CDC for whole-genome sequencing and antimicrobial susceptibility testing.
- Contact CDC at meningnet@cdc.gov with any questions or concerns about increasing meningococcal disease cases in their jurisdiction or outbreak investigation or control measures.
Recommendations for Healthcare Providers
- Maintain a heightened suspicion for invasive meningococcal disease and start immediate antibiotic treatment for persons with suspected meningococcal disease. Blood and cerebrospinal fluid (CSF) cultures are indicated for patients with suspected meningococcal disease [1].
- Recognize that invasive meningococcal disease may affect people of any age or demographic group.
- Current increases in disease are disproportionately affecting people ages 30–60 years, Black or African American people, and people with HIV.
- Be aware that patients with invasive meningococcal disease may present with bloodstream infection or septic arthritis and without symptoms typical of meningitis (e.g., headache, stiff neck).
- Ensure that all people recommended for meningococcal vaccination are up to date for meningococcal vaccines.
- All 11–12 year-olds should receive a MenACWY vaccine. Since protection wanes, CDC recommends a booster dose at age 16 years.
- For people at increased risk due to medical conditions (e.g., with HIV), recommended vaccination includes a 2-dose primary MenACWY series with booster doses every 3–5 years, depending on age.
- Immediately notify state, tribal, local, or territorial health departments about any suspect or confirmed cases of invasive meningococcal disease.
- Consult with your state or local health department for any questions about meningococcal disease treatment or contact prophylaxis, including any changes based on local meningococcal resistance patterns.
Recommendations for the Public
- Seek medical attention immediately if you or your child develops symptoms of meningococcal disease:
- Symptoms of meningitis may include fever, headache, stiff neck, nausea, vomiting, photophobia, or altered mental status.
- Symptoms of meningococcal bloodstream infection may include fever and chills, fatigue, vomiting, cold hands and feet, severe aches and pains, rapid breathing, diarrhea, or, in later stages, a dark purple rash.
- While symptoms of meningococcal disease can at first be nonspecific, they worsen rapidly, and the disease can become life-threatening within hours.
- Talk to your healthcare provider about meningococcal vaccines that may be recommended for you and your household or family members, including any recommended booster doses.
For More Information
- Health departments
- Meningococcal Disease Surveillance | CDC
- Meningococcal Disease | Manual for the Surveillance of Vaccine-Preventable Diseases | CDC
- Meningococcal Disease Outbreaks and Public Health Response | CDC
- Selection of Antibiotics as Prophylaxis for Close Contacts of Patients with Meningococcal Disease in Areas with Ciprofloxacin Resistance — United States, 2024
- Healthcare providers
- Everyone
- Signs and Symptoms | Meningococcal Disease | CDC
- Meningococcal Vaccination | CDC
- Visit CDC-INFO or call CDC-INFO at 1-800-232-4636
References
- American Academy of Pediatrics. Summaries of infectious diseases: meningococcal infections. [Section 3]. In: Kimberlin DW, Barnett ED, Lynfield R, Sawyer MH, eds. Red book: 2021–2024 report of the Committee on Infectious Diseases. Itasca, IL: American Academy of Pediatrics; 2021:519–32.
- Mbaeyi SA, Bozio CH, Duffy J, et al. Meningococcal Vaccination: Recommendations of the Advisory Committee on Immunization Practices, United States, 2020. MMWR Recomm Rep 2020;69(No. RR-9):1–41. DOI: http://dx.doi.org/10.15585/mmwr.rr6909a1
- Rubis AB, Howie RL, Marasini D, Sharma S, Marjuki H, McNamara LA. Notes from the Field: Increase in Meningococcal Disease Among Persons with HIV — United States, 2022. MMWR Morb Mortal Wkly Rep 2023;72:663–664. DOI: http://dx.doi.org/10.15585/mmwr.mm7224a4
The Centers for Disease Control and Prevention (CDC) protects people’s health and safety by preventing and controlling diseases and injuries; enhances health decisions by providing credible information on critical health issues; and promotes healthy living through strong partnerships with local, national and international organizations.
Department of Health and Human Services
HAN Message Types
- Health Alert: Conveys the highest level of importance about a public health incident.
- Health Advisory: Provides important information about a public health incident.
- Health Update: Provides updated information about a public health incident.
###
This message was distributed to state and local health officers, state and local epidemiologists, state and local laboratory directors, public information officers, HAN coordinators, and clinician organizations.
###